The Aortic Root as An Enthesis
Introduction
The aorta is the major blood vessel that is attached to the heart.
At the root or point of attachment to the heart, there is a specialised structure called the aortic valve.
The Seronegative Spondyloarthropathies and Ankylosing Spondylitis and Reactive Arthritis are associated with aortic root inflammation.
Aortic Root disease in Ankylosing Spondylitis/Reactive Arthritis is linked to the HLA-B27 gene since it is not typically seen in Psoriatic Arthritis [1]
Both the valve and the root of both can become diseased in arthritis patients.
Aortic root disease can occasionally be severe and may require valve replacement.
 |

|
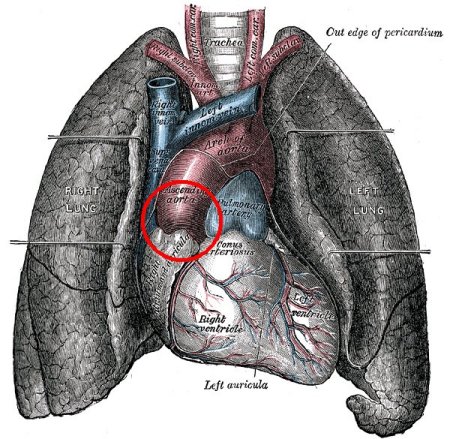
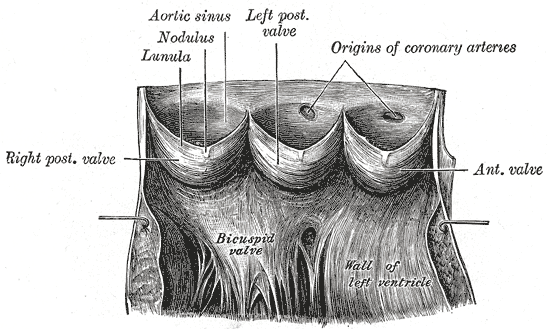
| The aortic root is the junction between the heart and circulation (inside red circle). Looked at from above and inside the artery it looks like the Mercedes-Benz logo with three flaps that open and close. The lower right image shows the complexity of the valve when the artery is cut open. Like joint insertions, this structure is subject to repeated stressing and microdamage and like insertions It is capable of self repair but this can go wrong resulting in disease. | |
Pathology
Like the entheses network in the skeleton this large valve enthesis shares several features including:
- Repeated cyclical motion- this motion is linked to the pumping of an estimated 200,000,000 litres of blood over an 80 year lifetime!
- This is inevitably associated with repeated micro damage and the need for associated repair responses.
A recent animal model study showed that over expression of a pro-inflammatory molecule called IL-23 lead to arthritis starting at the enthesis in the joints and aortic root disease also [2].
Like enthesitis in the skeleton the role of mechanical stress is recognised in aortic root and valve disease.
 |

|
| In the 1984 Textbook on Spondyloarthropathy the pre-eminent English Pathologist Eric Bywaters stated "Thus, it is tempting to suppose tht smooth-muscle sheath and its insertional soft tissue, the attachments for smooth muscle in the aorta or the arteries, or the attachment area of cartilage collagen fibers modified for stress or tension of movement at their attachment to bone might form the basis for an overall pathogenetic theory". He was the first person to correctly identify that mechanical stressing of the aortic valve and the enthesis could lead to pathology. | |
The similarities between the aorta and the enthesis doesn't end there. Cartilage develops in the skeleton in response to the patterns of stress and oxygen availability with this cartilage subsequently converting to bone. Likewise cartilage can develop in the aortic root and also be converted to bone [3].
| |
| In 2001 the shared common features of stress at the enthesis and the aortic root was also suggested to be responsible for eye disease and psoriasis over the elbows and knees. Occasionally disease can also occur at the apex or tip of the lungs in Ankylosing Spondylitis [4] | |
Key Clinical Considerations
Studies using cardiac ultrasound have reported a remarkably high frequency of aortic valve disease in Ankylosing Spondylitis [5, 6].
The cardiac ultrasound findings mirror joint ultrasound findings where low grade damage of non-symptomatic entheses is also common in Ankylosing Spondylitis.
In the case of Reactive Arthritis, heart block can occasionally occur due to the inflammation spreading out into the adjacent tissues that carry the nerves that regulate the heart beat.
Evidence suggests that aortic root damage is linked to the duration of Ankylosing Spondylitis [5, 6]
.Early studies suggested a link between valve disease and Ankylosing Spondylitis severity [4] but later studies using more sophisticated scanners did not show a link [6].
In keeping with the reparative nature of entheseal structures the aortic root abnormalities can resolve in up to a fifth of patients [6].
Aortic Root Disease in HLA-B27 gene positive patients without Arthritis
Aortic Valve and Root disease can occur in isolation without Arthritis (Reference 7).
Patients can develop a leaky valve or problems with cardiac conduction due to the process spreading into the nerves of the heart [7].
These cardiac problems are associated with carriage of the HLA-B27 gene. This gene is also present in over 95% of Ankylosing Spondylitis cases.
This strongly suggests that isolated aortic valve disease is an inflammatory enthesitis related pathology in a subset of patients with leaky valves.
Thus far Cardiologists and Rheumatologists have not explored how this could be potentially treated and reversed with modern effective biological therapies.
Key Considerations for Arthritis Patients
The valve disease is uncommon and is usually a late manifestation of Ankylosing Spondylitis.
Although aortic valve disease is well recognised in Ankylosing Spondylitis most doctors do not carry tests if the patient has no symptom.
Doctors periodically should listen to the hearts of Ankylosing Spondylitis cases to check for murmurs that are due to valve leakage.
If shortness of breath of chest pain develop then medical advice should be sought.
References
