The Proximal Interphalangeal (PIP) Joint in Psoriatic Arthritis
Introduction
The PIP joint is commonly involved in Psoriatic Arthritis (PsA). This page explains PIP disease. Disease at this site is very important since the Rheumatologist must distinguish it from osteoarthritis and Rheumatoid Arthirits (RA).
|
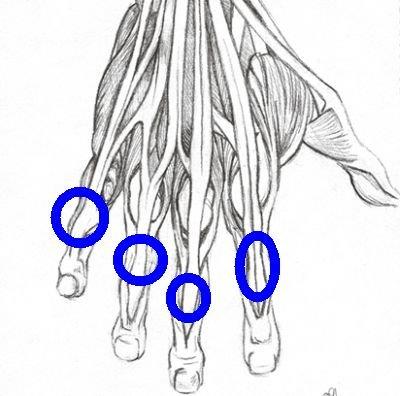
| Each hand and foot has 4 PIP joints (location shown inside the blue circles). These joints are commonly involved in all major types of arthritis including rheumatoid arthritis, osteoarthritis and psoriatic arthritis. |
PIP joint swelling
In PsA, PIP joint disease is often associated with diffuse swelling that extends well beyond the joint space. This was first explained by Radiologists from Croatia who showed prominent abnormalities at the PIP entheses on MRI scanning [1].
|
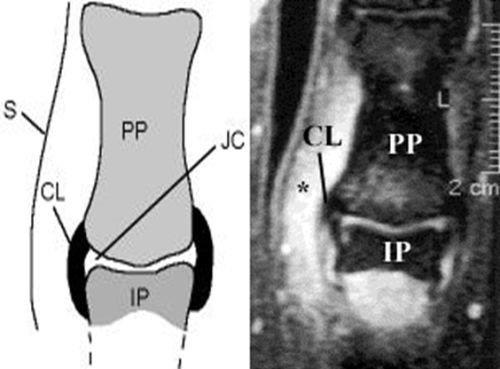
| The graphic on the left shows a cartoon of the joint anatomy and the right shows PIP disease in PsA. The diffuse swelling that is seen outside the PIP joints in PsA is linked to capsular enthesitis. This manifests as swelling that spreads away from the joint and is not centered on the joint space. S= skin. CL= collateral ligament and enthesis. JC= joint cavity. PP= proximal phalynx. IP = intermediate phalynx. The asterisk shows that the joint swelling is due to inflammatory changes outside the joint cavity related to the joint capsule and enthesis. |
Disease at this site may involve only one PIP or many PIPs may be involved.
Strategy for PIP disease
Rheumatologists will do blood tests called Rheumatoid factor, ACPA (anti-CCP) and Antinuclear antibodies (ANA) to exclude other causes of arthritis.
An X-ray of the joint may be performed to look for evidence of PsA or alternative conditions such as osteoarthritis (OA). Unfortunately in early arthritis, all of the blood tests may be negative and the X-ray may not yet show damage.
X-rays of the PIP joints pre and post therapy are often used to determine whether new therapies can prevent bone erosion or damage. This was historically important for drug licencing in PsA.
Ultrasound or MRI scanning may not reliably distinguish PIP joint disease due to PsA or OA.
Implications
PIP joint disease in PsA is intimately associated with enthesitis in that joint.
References
